
Introduction
Head injuries, whether incurred from a minor fall or a severe accident, areno laughing matter. One of the most serious consequences of head trauma is the development of hematomas, pockets of blood outside the blood vessels. Two of the most common forms of brain hematomas are subdural hematoma and epidural hematoma, both of which can cause serious complications if not treated early.
While these two conditions might seem similar, they are actually quite different, from their causes and symptoms to the treatments that will help. It is important for anyone, not just medical professionals, to understand the differences between subdural and epidural hematomas, as these bleedings play a vital role in alerting people to the potential dangers of head injury.
What Is a Hematoma?
A hematoma is a localised collection of blood outside the blood vessels that results in a bruise. When it occurs in the brain, the pressure on brain tissue must be relieved as soon as possible to prevent lasting damage. Hematomas of the brain, both subdural bleeding or epidural and between the brain and its covering, the meninges.
Although the symptoms and etiologies may be similar, these are two unrelated haematomas with respect to their site of origin, responsible aetiology, and therapeutic approach.
Why Understanding Subdural and Epidural Hematomas is Important?
If you or a loved one has experienced a head injury, being able to identify the type of hematoma is vital for getting timely medical care. A subdural hematoma typically develops more slowly, often due to mild head trauma, and is common in elderly people or those on blood-thinning medications. On the other hand, epidural hematomas tend to develop rapidly after more significant trauma, such as a skull fracture, and can quickly lead to life-threatening pressure on the brain.
Knowing the signs, symptoms, and differences between these two types of hematomas can help prevent further injury and ensure prompt treatment. Delayed diagnosis and treatment can lead to permanent brain damage or even death.
This article will explore the essential differences between subdural and epidural hematoma, including their causes, symptoms, diagnosis, and treatment options. By the end, you will have a clearer understanding of these serious conditions and how they are managed in a clinical setting.
What is a Subdural Hematoma?
Subdural hematoma (SDH) is a form of traumatic brain injury in which blood gathers between the dura mater and the arachnoid mater layer of the meninges surrounding the brain. This collection of blood can put a lot of pressure on the brain and cause serious neurological complications if not managed properly.
Causes of Subdural Hematoma
A subdural hematoma is frequently the result of head trauma, suchas when the side-to-side movement of the brain against the skull ruptures small blood vessels. The most frequent causes include:
Falls: This type of hematoma can be especially common in the elderly, where fallsare more common and brain tissue becomes more delicate over time.
Auto Accidents: When a crash occurs, the brain is jolted, causing it to bounce against the inside of the skull, resulting in blood pooling between the dura mater and the brain.
Blows: Physical attacks that cause blunt trauma can result in a subdural hematoma.
Shaken Baby Syndrome: Infants have very delicate brain tissue; violent shaking can result in subdural hematomas.
In some cases, even mild head trauma can cause a subdural hematoma, particularly in individuals who are elderly or on blood-thinning medications, as these factors increase the risk of bleeding.
Symptoms of Subdural Hematoma
Symptoms of a subdural haematoma can be slow to develop and may take several hoursor weeks to appear. The slow progression of the disease is also one of the reasons that it can be hard to diagnoseat first. Common symptoms include:
• Headache: The most common symptom of a subdural hematoma isa constant headache.
• Fuzzy thinking: A person may appear more muddled in their thinking, or have memory problems or a lack of concentration.
• Dizziness: This can be anything from feeling lightheaded to being unable to stand or keepyour balance.
• Feeling Sick and Being Sick: You can get these symptoms if your brain swells.
• Unconsciousness, can still hear and feel: Unconsciousness is a sign of more severe cases, but it is not always present right away.
• Weakness or Numbness: Specifically on one side of the body, if thehematoma presses on specific parts of the brain.
Because age-related changes in the elderly and symptoms of mild cognitive impairment or dementia may mimic those of SDBHs, accurate clinical diagnostics are essential when individuals present symptoms following a head injury.
Diagnosis of Subdural Hematoma
To diagnose a subdural hematoma, doctors typically perform:
- Physical Exam: A thorough neurological examination to assess reflexes, cognitive function, and coordination.
- Imaging Tests: A CT scan or MRI of the brain is used to confirm the presence of a subdural hematoma and determine its size and location.
A CT scan is the most commonly used method for diagnosing an acute subdural hematoma, as it provides quick results. An MRI may be used to provide more detailed images, especially in chronic cases.
Treatment of Subdural Hematoma
Conservative Management:
- When the subdural hematoma is small and not causing significant pressure on the brain, doctors may monitor it with regular imaging tests to ensure it doesn’t worsen.
- Medications may be prescribed to manage symptoms such as headaches or nausea.
Surgical Intervention:
If the hematoma is large or causing significant pressure on the brain, surgery may be required to remove the accumulated blood and alleviate pressure. The most common surgical options include:
- Craniotomy: A surgical procedure where a portion of the skull is removed to access and remove the blood clot.
- Burr Hole Drilling: A less invasive option, where small holes are drilled into the skull to drain the blood.
Prognosis of Subdural Hematoma
The prognosis of a subdural hematoma can vary depending on several factors, including the hematoma’s size, the time to treatment, and the patient’s age and overall health.
- Acute subdural hematomas (which occur suddenly) are more dangerous and may require immediate surgery.
- Chronic subdural hematomas (which develop slowly over time) may cause milder symptoms but can still be life-threatening if left untreated.
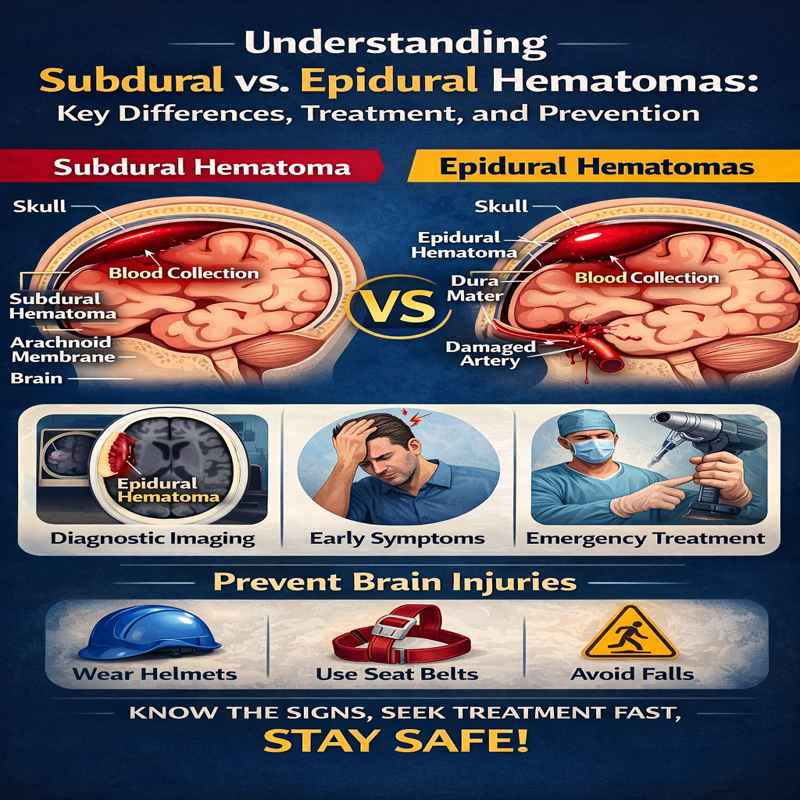
Key Differences Between Subdural and Epidural Hematomas
While subdural and epidural hematomas are both types of brain bleeds, they differ significantly in several key areas, including location, causes, symptoms, and treatment. Understanding these differences is crucial for diagnosing and treating each condition effectively.
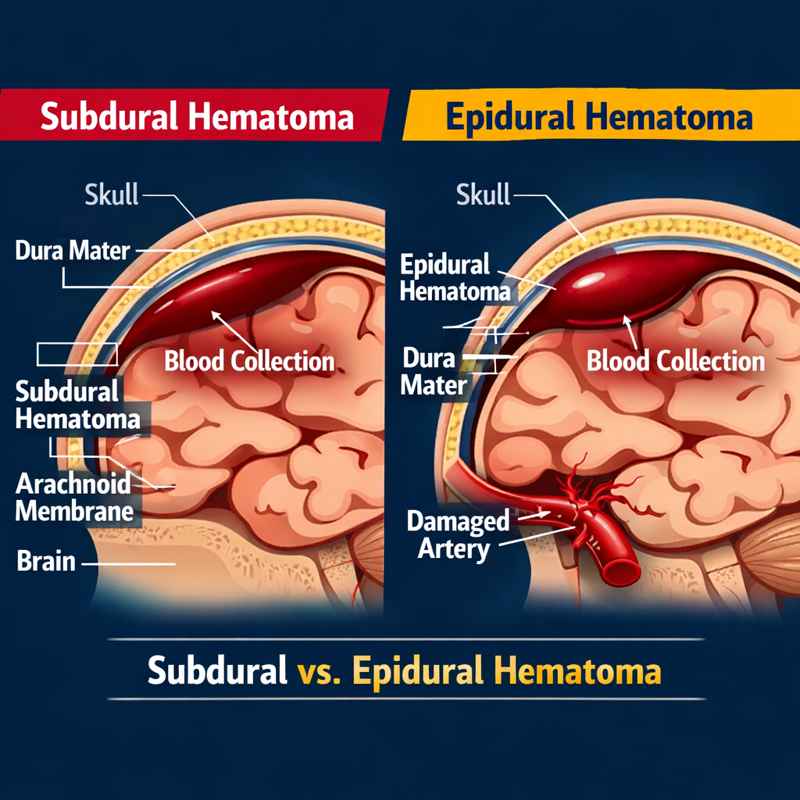
1. Location
- Subdural Hematoma (SDH): A subdural hematoma occurs between the dura mater (the outermost layer of the brain’s protective covering) and the arachnoid membrane (the middle layer). This type of hematoma typically affects the brain directly, as blood accumulates in the space between these two membranes.
- Epidural Hematoma (EDH): An epidural hematoma occurs between the dura mater and the skull. It is generally located outside the brain, where blood collects between the dura mater and the inner surface of the skull.
2. Causes
- Subdural Hematoma: Subdural hematomas are most often caused by head trauma, particularly from falls, car accidents, or assaults. These can occur even with minor head injuries, especially in elderly individuals or people on blood-thinning medications.
- Epidural Hematoma: Epidural hematomas are primarily caused by blunt trauma to the head, which often results in a skull fracture. The most common cause is a severe blow to the head, such as from a car accident, a sports injury, or an assault. These injuries usually tear the middle meningeal artery, causing rapid bleeding.
3. Onset of Symptoms
- Subdural Hematoma: Symptoms of a subdural hematoma often develop gradually, sometimes taking hours to days after the initial trauma. The onset can be slow, and in chronic cases, symptoms may not appear for weeks or even months. This makes subdural hematomas harder to detect in the early stages, particularly in elderly individuals or those with delayed reactions to head injury.
- Epidural Hematoma: Symptoms of an epidural hematoma typically develop rapidly, often within minutes to hours of the head injury. The condition is characterised by a lucid interval, during which the patient briefly regains consciousness and may seem fine, followed by rapid deterioration in consciousness as the hematoma enlarges and intracranial pressure rises.
4. Symptoms
- Subdural Hematoma: Symptoms of a subdural hematoma can include:
- Headaches
- Confusion or memory loss
- Nausea and vomiting
- Dizziness or loss of balance
- Gradual loss of consciousness (in severe cases)
- Weakness or numbness on one side of the body
- Slurred speech
- The symptoms of a subdural hematoma can worsen slowly, and in chronic cases, the condition may be mistaken for cognitive decline or ageing-related issues.
- Epidural Hematoma: Symptoms of an epidural hematoma often appear quickly and can include:
- Severe headache
- Loss of consciousness, followed by a brief period of alertness (lucid interval)
- Nausea and vomiting
- Dizziness and confusion
- Seizures (in severe cases)
- Hemiparesis (weakness on one side of the body)
- Epidural hematomas often result in more dramatic, acute neurological changes, and immediate medical intervention is essential to avoid fatal outcomes.
5. Diagnostic Methods
- Subdural Hematoma: The diagnosis of subdural hematomas typically involves:
- CT scans: CT scans are the most common imaging tests used to detect subdural hematomas, as they provide quick results and can identify the size and location of the blood clot.
- MRI scans: In some cases, especially for chronic subdural hematomas, an MRI may be used for more detailed imaging.
- Epidural Hematoma: An epidural hematoma is typically diagnosed using:
- CT scans: CT scans are also the first-line imaging tool for epidural hematomas, as they can quickly identify the characteristic lens-shaped or biconvex appearance of the hematoma.
- MRI scans: An MRI may also be used for further evaluation, especially if the CT scan is inconclusive.
6. Treatment
- Subdural Hematoma: The treatment for subdural hematomas depends on the size, location, and severity:
- Conservative treatment: In mild cases, the hematoma may be monitored with regular imaging, and medications may be used to manage symptoms.
- Surgical intervention: If the hematoma is large or causing significant pressure on the brain, surgery may be required to remove the blood clot. Craniotomy and burr hole drainage are common surgical procedures.
- Epidural Hematoma: Treatment for epidural hematomas typically requires immediate surgery:
- Craniotomy: The primary treatment for large or acute epidural hematomas is craniotomy, where a portion of the skull is removed to access and remove the blood clot.
- Burr hole drainage: In some cases, a less invasive procedure called burr hole drainage may be performed to evacuate the blood and relieve pressure on the brain.
7. Prognosis
• Subdural Hematoma:
The outlook of subdural hematoma can vary depending on the size of the bleed, how quickly it was diagnosed, the line of treatment, and the overall health or age of the patient. Chronic subdural hematomas have a better outcome with early treatment, whereas acute ones may necessitate aggressivemanagement and surgical intervention.
• Epidural Hematoma:
The outlook with epidural hematomas is usually better when treatment is given quickly. A high survival rate is reported when early surgical intervention is performed. But, if there is a delay in cure, the high rate of brain herniation and mortality occurs.
Diagnosis of Subdural and Epidural Hematomas
Prompt and accurate diagnosis is crucial for effective treatment and improving outcomes for patients with brain hematomas. Subdural hematomas (SDH) and epidural hematomas (EDH) require distinct diagnostic approaches, although both are identified on imaging. Understanding the differences in their diagnostic methods helps healthcare providers to choose the best course of action.
1. Clinical Examination
A physician will conduct a neurological examination to assess alertness, motor responses, and reflexes before testing. Symptoms such as headache, confusion, dizziness, nausea, or loss of consciousness may further raise suspicion. The doctor will also look for signs of brain damage, such as limb weakness or numbness, slurred speech, and problems with eyesightor coordination.
Important signs to consider:
- Subdural Hematomas: Symptoms may develop gradually and often result in confusion, headache, and weakness.
- Epidural Hematomas: Rapid onset of symptoms, including loss of consciousness and a lucid interval, typically follows a traumatic event.
2. Imaging Tests for Diagnosis
Imaging is the most reliable method for diagnosing subdural and epidural hematomas. The two most commonly used imaging techniques are CT scans and MRIs. Both tests can provide clear images of the brain and detect the location and size of the hematoma.
CT Scan:
- The CT scan is the most widely used imaging test for diagnosing brain hematomas. It is particularly effective for detecting acute subdural and epidural hematomas, as it is quick, non-invasive, and widely available. A CT scan can reveal the shape, size, and location of the hematoma, helping doctors determine the severity of the condition.
- Subdural Hematoma (SDH): On a CT scan, a subdural hematoma typically appears as a crescent-shaped area of blood between the brain and the dura mater.
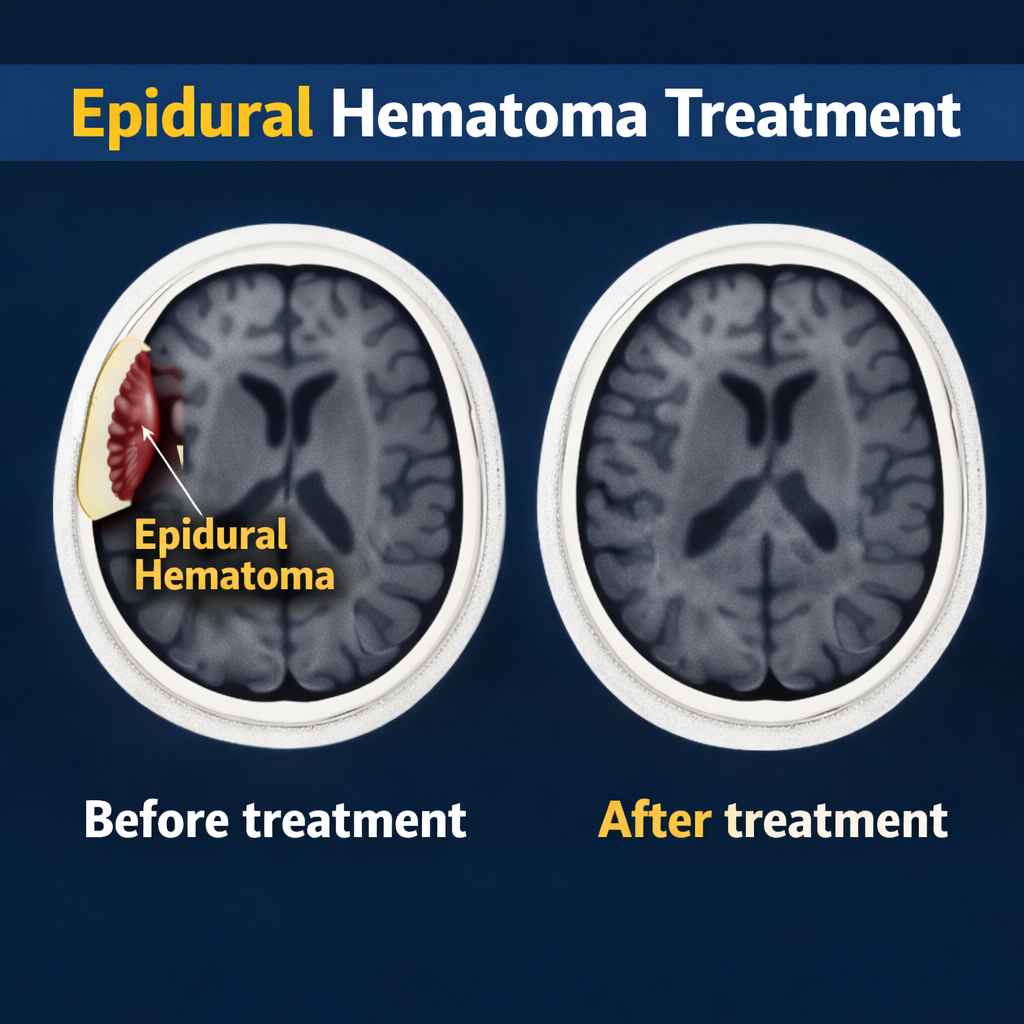
- Epidural Hematoma (EDH): Epidural hematomas show up as lens-shaped or biconvex collections of blood between the dura mater and the skull.
MRI (Magnetic Resonance Imaging):
While CT scans are ideal for emergencies, MRIs offer greater detail and are often used for diagnosing chronic subdural hematomas or for cases where CT scans are inconclusive. MRIs are particularly effective at detecting small or less obvious hematomas that may not be easily visible on a CT scan.
3. Time Factor in Diagnosis
• Acute Subdural Hematomas:
In acute subdural haematomas, the blood is often fresh and is seen on both CT and MR imaging. Such hematomas demand an immediate solution to avoid the latter of brain injury. If a patient is suspected of an acute subdural hematoma, doctors will try to perform a CT scan so they can make a rapid diagnosis.
• Chronic Subdural Hematomas:
Subdural hematomas recur over a longer period of time. In these cases, the blood has sometimes had time to organise and resorb, so that the hematoma may no longer be visible. Vic on CT. In chronic situations, MRI, which reveals more information about older blood collections, is more commonly used.
• Epidural Hematomas:
Because of the rapid evolution of symptoms in epidural hematomas, diagnosis ismade soon after the injury. CT scans are very good at detecting acute epidural hematomas, as they typically show the classic lens-shaped pool of blood.
4. Differential Diagnosis
Sometimes, other conditions need to be ruled out to confirm the presence of a hematoma. Conditions that may be considered during differential diagnosis include:
- Brain Tumours: Some brain tumours can cause similar symptoms (headaches, dizziness, nausea) and may appear as abnormal growths on imaging tests. However, hematomas can often be distinguished from tumours based on their location, shape, and the history of recent trauma.
- Intracerebral Haemorrhage: In cases of bleeding within the brain tissue itself, a CT scan will show a different pattern of blood accumulation than a hematoma located between the brain and the skull.
5. Other Tests and Monitoring
• Intracranial Pressure Monitoring:
For subdural and epidural hematomas, a doctor can perform intracranial pressure (ICP) monitoring to measure the pressure on the brain. The increased ICP may indicate that the hematoma is growing and requires treatment.
• Blood Tests:
While blood tests cannot directly diagnose a hematoma, they can provide valuable information about an individual’s health. Blood tests can also be useful for assessing your ability to clot (especially in patients taking an anticoagulant) and for helping providers understand the severity of your brain injury.
6. Importance of Early Diagnosis
Early diagnosis and prompt treatment are crucial to improving the prognosis of both subdural and epidural hematomas. If either condition is left untreated, it can result in severe neurological damage, permanent disability, or even death. The sooner a hematoma is diagnosed, the sooner treatment can begin, thereby significantly improving the patient’s outcomes.
Treatment of Subdural and Epidural Hematomas
The treatment for subdural and epidural hematomas varies depending on their severity, size, and location. Both conditions can cause significant pressure on the brain, leading to life-threatening complications if not addressed quickly. Understanding the treatment options for each type of hematoma is essential to ensuring the best possible patient outcome.
1. Treatment of Subdural Hematoma
The treatment for subdural hematomas depends on whether the condition is acute (rapidly developing) or chronic (slowly developing). Here’s how doctors typically manage each type:
- Acute Subdural Hematoma: Acute subdural hematomas are a medical emergency, and immediate treatment is required. The primary goals are to remove the blood, relieve pressure on the brain, and prevent further brain damage.
Surgical Options:
o Craniotomy: The typical operation for acute subdural hematomas, a craniotomy is the removal of part of the skull to allow access to the brain so that blood can be removed. It is typically performed for a large hematoma that creates a significant mass effect on the brain.
o Burr Hole Surgery: Burr hole surgery can be performed in selectpatients. A tiny hole is drilled through the skull to let blood escape and ease pressure on the brain. Itis usually performed with a small hematoma or in critically ill patients.
Medications: In addition to surgery, patients may be given medications to manage symptoms, reduce brain swelling, and prevent complications such as seizures. Medications like mannitol or steroids may be used to reduce intracranial pressure.
Postoperative Care: After surgery, patients are closely monitored in an intensive care unit (ICU) for any signs of worsening symptoms, including changes in neurological function. Regular CT or MRI scans may be performed to ensure the hematoma does not recur.
Treatment Options:
- Surgical Drainage: If the hematoma continues to grow or causes significant symptoms, surgical drainage may be necessary. This is often done with a burr hole procedure, in which a small hole is drilled into the skull, and the blood is drained. In some cases, a catheter is placed to allow continuous drainage.
- Mild Cases: In some patients with small chronic subdural hematomas and no severe symptoms, doctors may choose a conservative approach of regular monitoring and observation, with treatment only if symptoms worsen.
2. Treatment of Epidural Hematoma
Epidural hematomas are usually more acute and develop quickly after a head injury. Immediate medical intervention is critical to prevent brain damage or death.
- Craniotomy: Craniotomy is the primary surgical treatment for epidural hematomas, especially when a large blood collection or increased intracranial pressure is present. The surgeon removes a portion of the skull to access the hematoma and evacuate the blood. This procedure is typically done as soon as the diagnosis is confirmed, especially if the hematoma is large or rapidly growing.
- Burr Hole Drilling: In some cases, especially if the hematoma is small or the patient is at high risk of complications from a larger surgery, a burr hole can be drilled to drain the blood. This technique is minimally invasive and can be effective in removing smaller hematomas.
Medications:
- Sedation and Pain Management: Patients undergoing surgery for epidural hematomas are usually sedated and may be given pain medications before and after surgery to manage discomfort.
- Anti-seizure Medications: If the patient has a seizure or is at risk for seizures, anti-seizure medications such as phenytoin may be used to prevent further neurological complications.
- Post-Surgery Care:
- After surgery, patients are closely monitored in an ICU to observe for any signs of brain swelling or reaccumulation of blood. Additional imaging studies, such as CT or MRI scans, are performed regularly to ensure the hematoma has been fully evacuated and that no further bleeding is occurring.
3. Treatment Goals and Approach
- Reducing Intracranial Pressure (ICP): One of the main goals in treating both subdural and epidural hematomas is to reduce pressure on the brain. High ICP can lead to brain herniation, which is a life-threatening condition that requires immediate treatment.
- Prevention of Complications: Both subdural and epidural hematomas can lead to secondary complications, such as infection, seizures, or neurological deficits. Preventive treatments, such as antibiotics and anti-swelling medications, are often used to reduce the risk of complications.
- Rehabilitation: Depending on the severity of the hematoma and the resulting brain injury, patients may require long-term rehabilitation. This can include physical, speech, and cognitive therapy to help restore lost functions and improve quality of life.
4. Prognosis of Hematomas and Post-Treatment Care
- Subdural Hematomas:
- The prognosis for acute subdural hematomas depends largely on the speed of diagnosis and treatment. Early intervention typically leads to a better outcome, although there may still be long-term neurological effects.
- For chronic subdural hematomas, the prognosis is generally more favourable, especially when caught early. With treatment, many people recover without significant long-term effects, though some may experience cognitive or physical impairments.
- Epidural Hematomas:
- Epidural hematomas have a better prognosis when surgery is performed promptly, with many patients making a full recovery if treated within the first few hours of the injury.
- If surgery is delayed, the prognosis can worsen due to the rapid increase in intracranial pressure, which can lead to brain herniation and permanent brain damage or death.
Prevention of Subdural and Epidural Hematomas
While it is not always possible to prevent brain injuries, several measures can reduce the risk of developing both subdural and epidural hematomas. By understanding the factors that contribute to these injuries and implementing preventive strategies, individuals can reduce their risk of experiencing these potentially life-threatening conditions.
1. Preventing Subdural Hematomas
Subdural hematomas are often caused by head trauma, which may result from falls, car accidents, or other types of blunt force injuries. Here are a few steps that can help reduce the risk:
- Fall Prevention:
- For the Elderly: Older adults are at a higher risk for subdural hematomas due to increased fragility of the brain tissue and higher likelihood of falls. To prevent falls:
- Install grab bars and non-slip mats in bathrooms.
- Use well-lit pathways and ensure that the home is free from obstacles that could cause tripping.
- Exercise regularly to improve balance and strength. Activities such as yoga or tai chi can improve coordination and reduce the risk of falls.
- Home Safety: Ensure that homes are equipped with handrails, secure carpets, and clear walkways to prevent tripping hazards.
- Footwear: Wearing appropriate shoes with good traction can help prevent falls, especially for older adults or those with mobility issues.
- Medication Management:
- Blood Thinners: People who take blood-thinning medications (such as warfarin or aspirin) should be aware of the increased risk of bleeding, including subdural hematomas. Regular medical checkups and consultation with a healthcare provider can help manage dosage and assess the risk of bleeding complications.
- Regular Monitoring: For individuals on blood thinners, regular monitoring of the blood’s clotting ability is essential. Medication adjustments may be needed if bleeding risk increases.
- Proper Head Protection:
- Helmet Use: Wearing helmets is a crucial preventive measure, particularly during activities such as cycling, skateboarding, skiing, and playing contact sports. Helmets help protect the head from injury and minimise the risk of traumatic brain injuries (TBIs).
- Safety Gear for Children: Ensuring children wear appropriate protective gear, such as helmets and knee pads, can significantly reduce the risk of falls that lead to subdural hematomas.
2. Preventing Epidural Hematomas
Epidural hematomas are often caused by significant head trauma, such as skull fractures resulting from car accidents, sports injuries, or assaults. Since these injuries are often severe and involve rapid bleeding, prevention can focus on reducing the likelihood of trauma.
- Car Safety:
- Seat Belts: Always wearing a seat belt while in a vehicle is one of the most effective ways to prevent head injuries in a crash. Seat belts reduce the risk of head trauma and prevent the body from being thrown around during sudden decelerations or collisions.
- Child Safety Seats: Ensuring that children are securely placed in appropriate car seats based on their age and weight is essential for protecting them from head injuries in case of an accident.
- Sports and Physical Activity:
- Helmet Use: Wearing helmets is crucial in contact sports (e.g., football, hockey) and other high-risk activities (e.g., biking, skateboarding). Helmets help protect against skull fractures and epidural hematomas by absorbing the impact from blows to the head.
- Proper Training and Supervision: Athletes should undergo proper training to learn safe techniques that reduce the risk of head injuries. Coaches and parents should ensure that children and young athletes follow appropriate safety guidelines and avoid risky play that could result in head trauma.
- Workplace Safety:
- In certain professions, such as construction or factory work, wearing proper protective gear, including hard hats, can prevent skull fractures and reduce the risk of epidural hematomas.
- Workplace Safety Training: Employers should provide safety training to workers, emphasising the importance of following safety protocols to minimise the risk of head injuries.
3. General Injury Prevention Strategies
- Regular Exercise and Fitness:
- Maintaining physical fitness through regular exercise can improve overall strength, balance, and coordination, helping prevent falls and other injuries. Strengthening the neck and upper body muscles can also help protect against neck and head trauma during falls.
- Awareness and Education:
- Public Education Campaigns: Public health campaigns that raise awareness about the risks of head injuries and promote safety measures, such as wearing helmets and using seat belts, can help reduce the incidence of both subdural and epidural hematomas.
- Injury Prevention Programs: Schools, community centres, and sports organisations can implement programs to educate children, teens, and adults about the importance of safety during physical activities and how to prevent head injuries.
4. Post-Trauma Monitoring
You need to be able to recognise it, even if you’ve only experienced a light bump on the head. Looking for symptoms such as a persistent headache, nausea, confusion, or drowsiness can help identify them before they become more serious.
Conclusion
Finally, both subdural and epidural haematomas are criticalneurological problems demanding early diagnosis and intervention. Even thoughthey have a lot of commonality, including the dangers both pose to inflicting serious brain damage if not promptly recognised and appropriately treated, the two conditions are quite different in origin, symptomatology, and treatment.
Subdural hematomas are caused by head injuries and cause more gradual symptoms that make early detection harder. Chronic subdural hematomas are a specific cause of chronic pain after brain injury. It can take weeks to develop and not make themselves known until they begin producing symptoms of Swoyer’s injuries. Early diagnosis using imaging tests like CT scans or MRIs is essential to deciding whether surgery or more conservative management is necessary.
They tend to be the result of a major head injury (such as a skull fracture), and they develop quickly; frequently, there is an obvious interval, also known as a lucid interval, then loss of consciousness. It most often requires surgery to remove the blood and decrease pressure on the brain. CT is the gold standard for diagnosis of epidural haematomas and early treatment can result ina favourable outcome.
“Both conditions underscore the critical need to prevent head injury, particularly in high-risk activities such as driving, playing sports, or workingon the job in settings where an injury could occur to the head.” Helmets, seat belts, and preventative measures against falls can significantly reduce the risk of developing these deadly conditions.
Finally, knowing the signs is critical for early diagnosis and treatment, which can be lifesaving. If you or anyone you know has had a head injury and is experiencing symptoms such as confusion, severe headache, or dizziness, it is vital to get the patient to medical care immediately and rule out a hematoma for a good chance at recovery.